Communicator Reality...where framing this in terms of a "medical issue" misses the boat big time!!!!7/19/2021 So you go to the hospital, or the doctor, or even a Speech-Language Pathologist (gasp!!!!!) and one of these lovely professionals tells you what it is that is wrong with you....what broke in terms of your communication or swallowing. This is the medical model in which we gather information, compare it to what we know, narrow down a diagnostic label, tell you what it is, and give you options about how to treat "it". My website is full of the influence of this medical model....it is literally everywhere. Your insurance then dictates that when you get "treatment", it is associated with a diagnostic label...and it is YOU that has the appointment and gets treated. This might work well for a broken leg, but communication, voice, and even swallowing are much more nuanced because they exist within a social context. The medical model says the burden of a change in communication falls squarely on YOU...YOU the person with a condition or illness. BUT, this challenge has happened to you, your family, your social network, your social roles and identities (employment, cultural, other). There is both a "medical model system set-up" and an understandable temptation (that probably exists even independently of the influence of the medical model) to FIX IT---IT being whatever the labeled problems are (word-finding, grammar, vocal pain or tension, etc.). To fix those pieces that are different inside of you and in YOUR messages. And certainly this can be a PART of the puzzle, but it would be terribly narrowly-focused and ultimately less helpful for us to ignore the other pieces. What are those pieces you ask? Brace yourself for a busy visual!!!!  A change really means that expectations have not been met in some way.
We expected life to proceed in a certain way...and it didn't. We expected our communication to continue as it had always been...and it didn't. We have those communication expectations about ourselves and about others, and THEY have expectations about themselves and about you. Expectations when met make us feel safe because they are predictable---unpredictable things make us nervous. We use our senses to find out if expectations are being met or not. So let's assume that these two colorful people are interacting. They are using their senses to see if expectations are being met. This is all happening prior to and while an actual message is being communicated. Both of these people are constantly interpreting how the interaction is going: is it meeting expectations? how is the other one doing? how am I doing? If something seems to NOT meet expectations, this is where our thoughts come in. Our senses are on high alert and we start processing more...and this happens very quickly. The most efficient thoughts are the "broad-strokes" type thoughts that label and categorize, especially if you have no or limited personal experience with a certain reality...and stereotypes fall into this. So if you are speaking with someone, and they are struggling to find words, you recognize that this goes against your expectation, and now you have thoughts. These thoughts can be so varied, and they are hard to predict because we are all different. This is yet another level of unpredictability in this communication puzzle. We are not mind-readers, so we make guesses. These guesses may be: 1) maybe they don't know what they want to say, 2) maybe they don't know how to say it. Then we try to PLAN what we need to do about it: 1) do I need to help them in some way?, 2) how do I help them? Do I have TIME to help them? Then we might have some FEELINGS about it: 1) I'm really annoyed or maybe not annoyed but flustered because I don't know how to help. And then we actually DO something: 1) I roll my eyes, tap my feet, look around for someone you know to communicate FOR you. But this can go in another direction. The guess might be: 1) Oh, this person is having trouble communicating kind of like my grandpa. The FEELING might be: I love my grandpa. The PLAN might be: I have some ideas about how I can make this interaction better for both of us. The DO might be: I'll offer a pen and paper, offer verbal or written choices, etc. These are REACTIONS: the thoughts, feelings, the plans, and actions. Everyone in the interaction has them, everyone in the interaction makes ASSUMPTIONS and tries to INTERPRET what the OTHER'S INTERPRETATION and REACTIONS are, and these all influence our MESSAGES: what we share, when we share, where we share, and how we share it (stuttered, choppy, single words, use of drawings or pictures, etc). YES...successful communication is not equal to the mechanics of the message. In fact, successful communication can happen even if the mechanics of the message are not perfect, are not as expected, but because all of the other factors (the interpretations/thoughts, the feelings, the plans, and the do's) allow the communication to flow. IMPORTANTLY, a kink in any one of those cogs can make communication be interpreted as unsuccessful, AND a mechanically-changed message can still result in SUCCESSFUL COMMUNICATION (perceived by all involved as successful). What else do we bring to the table? It is more than just the interaction itself. Our experiences, including changes in communication, have an impact on our identity. We make decisions about whether or not a specific piece of our identity has relevance in a situation (for example, the fact that I have vocal cord nodules and need periodic voice breaks to have my voice serve me well during my day), and if we should share it or try to hide it. We analyze the type of situation we are in, what kind of talk is expected, what is our relationship with the other communicators in the interaction, how do we COMPARE to the other communicators in the room (usually we frame this in terms of better or worse, normal or changed---and we can explore together how these dichotomies are not very helpful). What risks and benefits are each of the communicators facing in 1) starting or continuing the interaction? or avoiding the interaction? This can be lots of things: humiliation, loss of job, access to healthcare, loss/access to participation in enjoyable activities, self-dignity. These all impact our communication interactions, and which interactions we choose to have or not have. It is helpful to try to take a step back and observe our own behavior here, with judgment. BOTTOM LINE: There are many pieces to the communication puzzle, and they are ALL impacted with a communication change. This does not exist solely within the individual, but within the social sphere. Communication and changes to communication are not just about the mechanics of the message delivery or the messages themselves.
0 Comments
When you look at the name of my business, it would be reasonable to wonder 1) what the heck does a Speech-Language Pathologist have to do with swallowing, and 2) oh wow! I had no idea that someone could have difficulty swallowing! These were thoughts I had myself when I started on my journey to become an SLP. What is swallowing all about?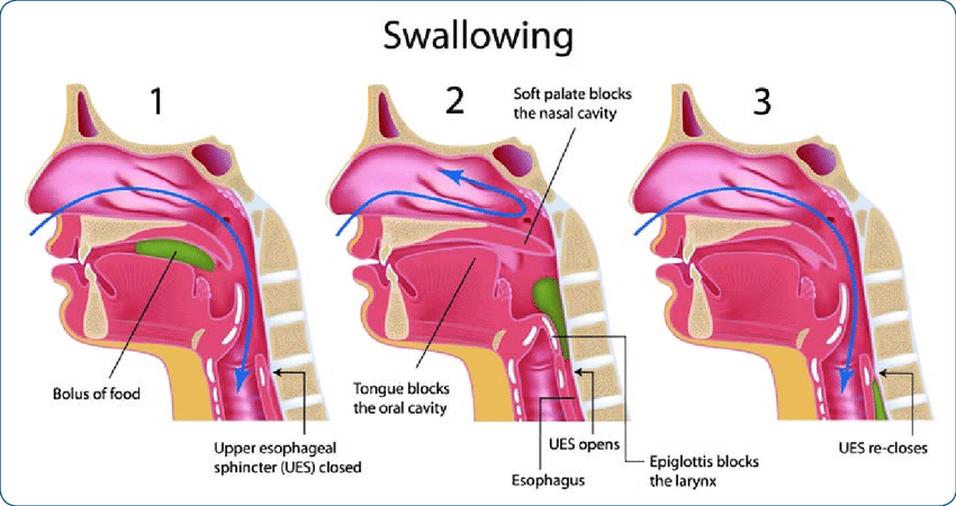 Miller, Karen & Plowman, Emily & Tabor Gray, Lauren. (2018). Living with ALS_Adjusting to Swallowing Changes and Nutritional Management. The pictures you see above are to be looked at in sequence as snapshots of time. Aside: The pictures may remind you of the picture presented in my 1st post on voice---the shared anatomy for voice & swallowing function is the primary reason WHY Speech-Language Pathologists play a role in joining you in facing swallowing problems!! Imagine this is your face sliced right down the middle and you are looking in at it from the side (I'm not sure how to word that to not make it sound gross!!!). To the far left, you see your nose and lips. Right behind the lips are your teeth and hard palate (in white). Your tongue is the pinkish mass attached to the bottom of your mouth (pictured behind the teeth). This image is a bit misleading, as the tongue attaches at its farthest point down in our throat, a bit farther down than the image suggests. If you move to the back of the mouth you see that there is an opening that goes up into the nose area, and then as you proceed downwards........ HOUSTON...WE HAVE A PROBLEM! Design flaw! Our throat divides into 2 tubes: our airway in the front (where that 1st blue arrow is pointing), which leads to the lungs, and the esophagus behind it that goes toward the stomach. We are anatomically set up to have problems with anything we put in our mouths (or anything that lives there...lots of bacteria) ending up in the lungs where it shouldn't be. We all have the occasional feeling that something tries to go down the wrong tube and we cough and cough and cough and that tickle is so annoying....but how is this prevented most of the time? How swallowing usually works...in a nutshell 1) We hold our breath when we swallow, and the breath cycle is paused at some point during our exhalation so that when we have finished swallowing, we finish breathing out. This is helpful so that just in case any of that food or liquid is still near the airway, the airflow is more likely to push it up and out rather than suck it in toward the lungs. 2) Our airway moves up and forward as we swallow. This literally gets it out of the way and opens that soft flexible tube in the back, the esophagus, to let food and liquid in. Do not rely on this picture to show you this, but you can get a sense of this yourself if you swallow your saliva right now. Place your fingers on your Adam's apple, and then swallow. Do you feel your Adam's apple bob up and then back down? That is your airway moving during swallowing! 3) OK, so now picture your saliva as the green blob in the pictures. By virtue of this movement, the handy flap of cartilage between the base of our tongue and the entrance of the airway flops over and covers the entrance to the airway. This cartilage, the epiglottis, is pictured as a rose thorn in the 1st picture, and folded over the airway in the 2nd picture. In this 2nd picture, you see the green blob of saliva or food bypassing the airway and entering the esophagus. 4) Our vocal cords, which are pictured as that lighter band at the top of the airway, close just in case anything should think about trying to enter the airway. Typically when we get that tickle feeling of something going down the wrong tube, it has entered that upper part of the airway, above or at the level of the vocal cords. Your cough response is generated by power from your lungs and your vocal cords opening and closing forcefully to move the material back up out of the area. How is the design flaw a recipe for swallowing challenges? https://www.reddit.com/r/CrappyDesign/comments/3umn8j/they_must_have_been_short_on_wall_parts/ Oh dear! So a privacy wall was built with the intention of having this bathroom be multifunctional, but SIGH...there are problems. Our throats are a bit like this. They were designed to take care of swallowing, breathing, and vocal functions, but alas...things can get a bit dicey. If any one or combination of the 4 components of swallowing goes a bit haywire, trouble can start. There are many ways we can have challenges with swallowing! It is actually more amazing when we DON'T than when we DO! Some possibilities: Please be aware that any listed symptoms may have a variety of specific causes, and need to be thoroughly evaluated by the correct healthcare professional to know how to proceed with managing them for YOU.
So what can be done when there is a problem?Unfortunately, we can't be recalled back to the factory to request an anatomical fix for the flaw!! So what are our options? First, let your doctor or healthcare provider know you are having trouble with your swallowing. They will be able to determine if an SLP may be the right professional to join you on your journey to manage the challenge. Other investigations & treatments may be more appropriate, at least as a first step, depending on the specifics of your situation. If a consultation with an SLP is recommended, the following options (in isolation or in combination) might be considered at your evaluation.
1) Posture changes during the swallow or establishing new swallowing habits, including targeted oral care practices (protect teeth/dentures, manage bacteria) and mealtime strategies. 2) Modifications to food & liquid to change how it is managed in the mouth & throat. In some very specific circumstances, this may mean bypassing the mouth & throat altogether. 3) Exercises to strengthen respiratory muscles that play a critical role in airway protection for swallowing. 4) Exercises for mouth & throat muscles involved in swallowing. These are sometimes used to try to prevent expected swallowing issues stemming from upcoming or ongoing medical treatments, improve swallow function after it changed as a result of an injury or illness, or slow down or better manage the progression of swallow challenges that go hand-in-hand with a progressive disease process. Each of the above has the potential for risks/limitations & benefits, and these should be discussed openly and thoroughly with your SLP as you work together to design a plan to adequately evaluate and treat your swallowing challenges. The plan may evolve over time if needed and should promote your health & well-being while respecting your goals, values & autonomy. Welcome!! I would like to preface this post by referencing highly valuable sources of information on this topic. To name a few: www.transplaining.info and prismaticspeech.com/. This post has been designed to be an introduction to gender-affirming voice in a Q&A format. What is the voice and how does it work?  Our vocal instrument is truly remarkable in that it boasts components of wind, string, and percussion instruments all in one. Our voice starts as a breath, our wind. Our diaphragm, a dome-shaped muscle that sits beneath our rib cage, contracts. It pushes down to allow for our lungs to expand, encouraging and accommodating air as it enters our bodies. When we exhale that air, muscles in our upper airway contract to form specific airway shapes that determine how quickly the air moves through, where air lingers, and where and how air escapes. Sound is achieved by a combination of 2-3 of the following mechanisms: 1) by the vibration and degree of tension vs. laxness, and the amount of stretching/thinning vs. compression/thickening of our instrument's strings (the vocal folds in the throat, housed in our voice box behind our Adam's Apple), 2) by the turbulence of air moving through narrow passages (like between your upper teeth and lower lip for an /f/ sound, or between the tongue tip and the palate for an /s/ sound). Or sequences of stoppages & explosions of air, our instrument's percussion, created by closures like the lips together for /b/, or the tongue tip to the palate for /d/, and 3) by the shape and degree of muscle tension in the roomy spaces of our throats, mouths, and noses that allow for certain tones to be enhanced and others to be suppressed (resonator of a wind instrument). It is the sequence of these movements and configurations, shaping that air as it moves out of our bodies, that creates the beautiful concert of sound that is our voice! Are there differences in the vocal instruments of people assigned male at birth and people assigned female at birth? Prior to puberty, no. The source of differences occurs at puberty; and the determining factor is the form of hormonal puberty one undergoes, not one's sex assigned at birth. The larynx of someone undergoing male puberty lowers, lengthening the vocal tract. The vocal folds themselves also become longer and bulkier. Someone undergoing female puberty does not experience the same degree of larynx lowering, and has shorter vocal folds. If you think of handbells, the larger handbells produce a deeper, dark tone, and the smaller handbells produce a higher pitch, tinkling, bright tone. The general anatomic differences in our vocal instruments predispose us to differences in sound, but this is a very binary construct, and anatomical variations are not all explained by sex assigned at birth. We can have different sized mouths, differently shaped palates, and more, and this is not related to sex. Moreover, anatomy is not nearly the whole picture! Now you have me intrigued. How is that not the whole picture? When one thinks of the "gendered" nature of our voices, we often think of pitch (though there are features of our voices that may influence a listener's perception of gender MORE than pitch...). Fundamental frequency (f0), or a voice's average pitch, is expressed as a range in studies comparing cis men and cis women. While using the cisgender binary framework to analyze voice is certainly problematic, interestingly these studies have shown that cis voices do not fit into gender binary boxes: cis female and cis male pitch trends not only vary substantially across languages, but also within languages across countries, time, and ethnicity. An individual who speaks multiple languages can have different average pitches for each language! To further boggle your mind on this last point, the average pitches of a multilingual cis person do not necessarily match the average pitches of cis people of the same gender who speak only one of those languages (monolinguals). Wait...what?? In other words, I speak Italian and American English. But the fact that I speak two languages means that I may have a different average pitch when speaking Italian vs. English, and that my average pitches may not match those of cis women who speak only Italian or only English!!! For more information, see the fascinating section titled "The Effects of Physiology and Culture on Cisgender Pitch" in the reference listed below. Bottom Line? Average fundamental frequency or pitch data analyzed in a cisgender binary framework vary as a function of sociocultural factors. There are instances of cis female F0 in one language (American English, for example) overlapping considerably with cis male F0 in another language (Urdu, for example); our vocal instruments are capable of a range of pitches, and this isn't dictated by the gender binary construct or sex assigned at birth. Even an individual can boast multiple average speaking pitches based on the languages they speak! Our culture and socialization mold our pitch, transcending any anatomical or biochemical "predispositions". And this is just pitch! Our voices are products of both nature and nurture. While we can't be completely free of neither our anatomy and biochemistry (ex. hormones, etc.) nor our history of socialization and cultural immersion, we aren't confined by them either: we can learn to shape our voices to approach and even achieve a desired sound with targeted techniques and conditioning. Adler, R.K, Hirsch, S., Pickering, J. (2018) Voice and Communication Therapy for the Transgender/Gender Diverse Client (3rd ed). San Diego, CA: Plural Publishing, pp 142-145. What does gender affirming voice & communication guided exploration involve? I have chosen the label "guided exploration" as opposed to "therapy" to suggest a partnership, a collaboration. "Therapy" suggests rehabilitation after an injury, or fixing. A goal of aligning one's voice with one's gender identity typically occurs in the context of a healthy vocal mechanism. In that case, our work is NOT fixing the vocal instrument; rather, it may involve exploring different ways to sound/play the instrument. You will meet your vocal instrument, gain confidence in molding it, sounding it. We will navigate how to vary the shape and coordinate the different parts of your instrument, by manipulating muscles of the mouth, palate, throat, voice box, abdomen & chest, to achieve desired sounds in a way that meets your needs (what I call the 4 pillars: doability, sustainability, usefulness, & safety (which can have many meanings)). I don't know what it means to be YOU; if you wish, you can show me what that means for your voice. What we target is determined by you, your instrument, and your voice goals. There are certain vocal and speech parameters that are associated with a listener's perception of masculinity or femininity, BUT the nature and direction of our explorations and practice DO NOT NEED to be in pursuit of stereotypical gender binary qualities....unless that is YOUR goal, of course. You may incorporate features that mirror aspects of your identity that aren't gender-linked or give you the flexibility to have different "voices" in different situations. We will likely dedicate some attention to: pitch (the height or depth of your tone), resonance (shaping of your instrument to enhance certain sounds or sound qualities), intonation (the overall melody of connected speech) and possibly loudness, language, & articulation. Non-verbal communication explorations can also be targeted if you want.
|
AuthorThese are my SLP-related musings. I will come up with topics that I think are interesting, but will be relying on you to make suggestions! Sometimes when you have gained more knowledge or "answers" on a topic you forget what the good "questions" are!!!! Archives
July 2021
Categories |
 RSS Feed
RSS Feed
